Meniscus Surgery
OVERVIEW / ANATOMY | SIGNS AND SYMPTOMS | DIAGNOSIS | TYPES OF TEARS | TREATMENT | MENISCUS TRANSPLANTATION | WHAT IS A MENISCAL TRANSPLANT? | WHERE DOES THE DONOR TISSUE COME FROM | HOW IS IT DONE? | HOW LONG IS THE RECOVERY? | HOW SUCCESSFUL IS THE PROCEDURE? | FREQUENTLY ASKED QUESTIONS
OVERVIEW / ANATOMY
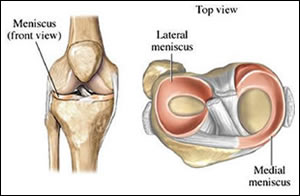
Figure 1 – Basic Anatomy
Meniscal tears in the knee are one of the most common orthopaedic injuries affecting patients of all ages. Each knee has an inner (medial) meniscus and an outer (lateral) meniscus (fig 1). Each meniscus is a piece of “C” shaped cartilage that is attached at the outside margins to the top surface of your lower leg bone (tibia). The thighbone (femur) comprises the top portion of the knee joint and sits on top of the menisci and tibia when standing. Your menisci have two important functions:
- They act as “shock absorbers” that protect the underlying bone and cartilage from wear and tear which can lead to arthritis.
- They help deepen the joint by virtue of their wedged shape and therefore add to the stability of the knee.
Athletes usually tear the meniscus while performing a twisting movement when the knee is bent or flexed. The inner (medial) meniscus is more commonly injured than the outer meniscus and often occurs in combination with injuries to other structures such as the Anterior Cruciate Ligament (ACL) and Medial Collateral Ligament (MCL). Older patients may also injure the meniscus without major trauma as the meniscus cartilage weakens with age.
SIGNS AND SYMPTOMS
Initially, you may experience a sharp pain or “popping” sensation. Most people can still walk on the knee after tearing their meniscus. Inflammation begins within a day and you may experience some or all of the following symptoms:
- Tenderness along the knee joint line.
- Stiffness and/or swelling.
- Clicking, popping, catching, or locking of the affected knee.
- Pain when walking down stairs.
The torn portion of the cartilage may rotate or flip into the joint space, causing it to catch or lock.
DIAGNOSIS
I will generally make the diagnosis of a meniscal tear based on how you injured the knee and the physical examination. I will order x-rays to look for osteoarthritis or other causes of knee pain. An imaging test called an MRI (Magnetic Resonance Imaging) may be ordered to visualize the soft tissue structures of the knee joint and confirm the diagnosis.
TYPES OF MENISCAL TEARS
The type of meniscus tear depends on the force and knee movement at the time of injury. Most commonly, younger athletes will tear the meniscus lengthwise if the femur and the tibia trap the meniscus when the knee rotates. This type of tear is referred to as a “bucket handle” tear (fig 2).
Figure 2 – Types of Meniscal Tears
Other types of tears include flap tears can be due to repetitive stress such as running. Older patients with degenerative changes tend to have transverse or horizontal tear types. Since the outer portion is the only part that receives any blood supply, it is likely that tears on the inside will not heal, therefore surgery is necessary.
TREATMENT
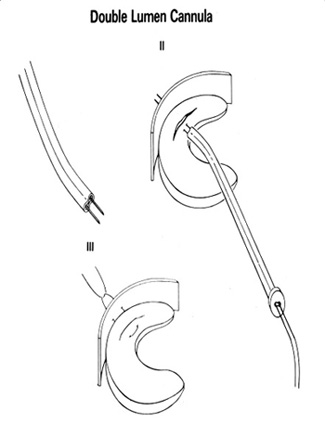
Conservative treatment of meniscal injuries begins with RICE. This acronym stands for Rest, Ice, Compression, and Elevation. This is especially important for the first 48 hours following the initial injury to decrease the pain and swelling of inflammation. I may also recommend that you take non-steroidal anti-inflammatory medications (NSAIDs) such as ibuprofen and naproxen. If you don’t have any symptoms such as locking, clicking, or pain you may not require surgery. The majority of the meniscus has a very poor blood supply, and does not heal. If pain or mechanical symptoms continue, surgical removal of the torn area of the meniscus is indicated. Using a minimally invasive surgery called arthroscopic surgery (fig 3), an arthroscope (a small camera that is about the size of a pencil) and other small tools of equal size, can fix the torn meniscus cartilage by removing or trimming just the damaged portion. Occasionally, I can repair a meniscus tear using sutures or absorbable plastic arrows or staples (Fig. 4).
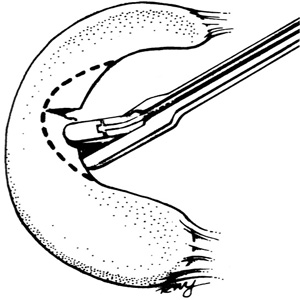
Figure 3 – Trimming of Arthoscopy
Following surgery you will start with crutches and usually discontinue them within a week. You may be required to complete a course of physical therapy. Rehabilitation is essential to help you regain balance, quadriceps and hamstring strengthening and regain normal function of your knee. Activity will increase when pain and swelling (inflammation from the skin arthroscopy incisions) decreases and motion (flexion and extension) of the knee increases.
MENISCUS TRANSPLANTATION
OVERVIEW / ANATOMY
If the meniscus is torn, I may be able to repair it or shave out a small portion, leaving most of your original tissue intact. In some cases, the meniscus can be extensively damaged and may need to be completely removed. Without the meniscus, the knee can develop persistent pain and swelling, and this accelerates the onset of degenerative arthritis.
If the patient is over 55, and is experiencing persistent pain and other arthritic symptoms, an artificial joint replacement may be an option. However, if the patient is physically active and under 50-55 years old, a procedure called meniscus transplantation may be an alternative. This procedure is relatively uncommon and is not recommended for all patients. If you do meet the criteria for the procedure, the benefits can be substantial.
WHAT IS A MENISCAL TRANSPLANT AND IS IT RIGHT FOR ME?
A meniscal transplant uses anatomically seized cadaver meniscus (allograft) from an authorized tissue bank to replace your removed meniscus. Patients who may be eligible for meniscal transplants must meet the following criteria:
- Physically active and under the age of 55.
- Missing more than 50% of their meniscus due to surgery, injury, or having a large tear that cannot be repaired.
- Persistent pain related to physical activity in the knee.
- The involved knee must have minimal evidence of arthritis.
WHERE DOES THE DONOR TISSUE COME FROM AND HOW SAFE IS IT?
The transplanted tissue comes from healthy human donors. The meniscal cartilage is frozen and sized by X-ray or MRI to fit the recipient. Currently, there is no synthetic or manufactured meniscal tissue.
The Food and Drug Administration (FDA) and the American Association of Tissue Banks (AATB) monitors the safety of the donor tissue. Prior to transplant, the meniscus is screened for any traces of infectious diseases such as Hepatitis B or C, or HIV/AIDS. Screening tests lower the odds of contracting any viral or bacterial disease to an extremely low level (less than 1 in a million), making this procedure very safe.
HOW IS IT DONE?
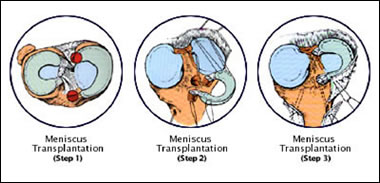
Meniscal Transplant
Meniscal transplant is a same-day surgery, which means you will be able to go home the same day of the surgery. It is performed with the arthroscope and a few small incisions are necessary, about 1cm in length, to fit the pencil-sized tools inside your knee to perform the surgery.The donor meniscus is secured into place with sutures where your old meniscus used to be, on top of the lower leg bone (tibia).
HOW LONG IS THE RECOVERY FROM A MENISCUS TRANSPLANT?
Everyone heals at different rates, but depending on your activity level, it may take 1-3 months to completely recover. For the first 2-3 weeks after surgery, you will use crutches and a knee immobilizer. This is very important to allow the transplanted tissue to become firmly attached to the lower leg bone (tibia). If you have a job that does not require too much activity (office, desk job for example), you may be able to return to work as soon as a week after surgery. If you are an athlete, it will take more time to return to the physical demands sports places on the body (3-6 months).
Physical Therapy and exercise are especially important. You can begin early weight-bearing exercises. In most cases, you can return to running after three to four months, but other activities that place such as squatting or bicycling may take up to six months after surgery to perform safely.
HOW SUCCESSFUL IS THE PROCEDURE?
About 80-90% of the time, meniscal transplants are effective in relieving pain and swelling. Because it is a relatively new procedure, long-term results have not been established. Pain relief with increased knee function are the goals of this surgery.
FREQUENTLY ASKED QUESTIONS
Click Here to view Frequently Asked Questions for Meniscus Surgery.